Breast Reconstruction Surgery
Serving patients in: Paramus, Wyckoff, Ridgewood, Allendale, Woodcliff Lake, Montvale, Saddle River, Upper Saddle River, Westwood, Ho Ho Kus, Park Ridge, Rivervale, Old Tappan, and surrounding areas.


At The Breslow Center for Plastic Surgery, we support The American Cancer Society’s “Making Strides against Breast Cancer.” Help and join The Breslow Center in the fight against breast cancer by visiting their website above.
A diagnosis of breast cancer can be an extraordinarily traumatic event. For many of these women, treatment with breast conservation surgery may be an option. For others, however, treatment with mastectomy may be the recommendation. Breast reconstruction surgery can help avoid the devastating psychological impact mastectomy can have on one’s self-image and self-confidence.
As recently as 25 years ago, options for post-mastectomy breast reconstruction were severely limited. Furthermore, the results of those procedures in use were generally unnatural and lacking. Fortunately, advances in plastic surgery since that time have enabled us to offer both single and double mastectomy patients several excellent options for breast reconstruction at our Paramus plastic surgery practice.
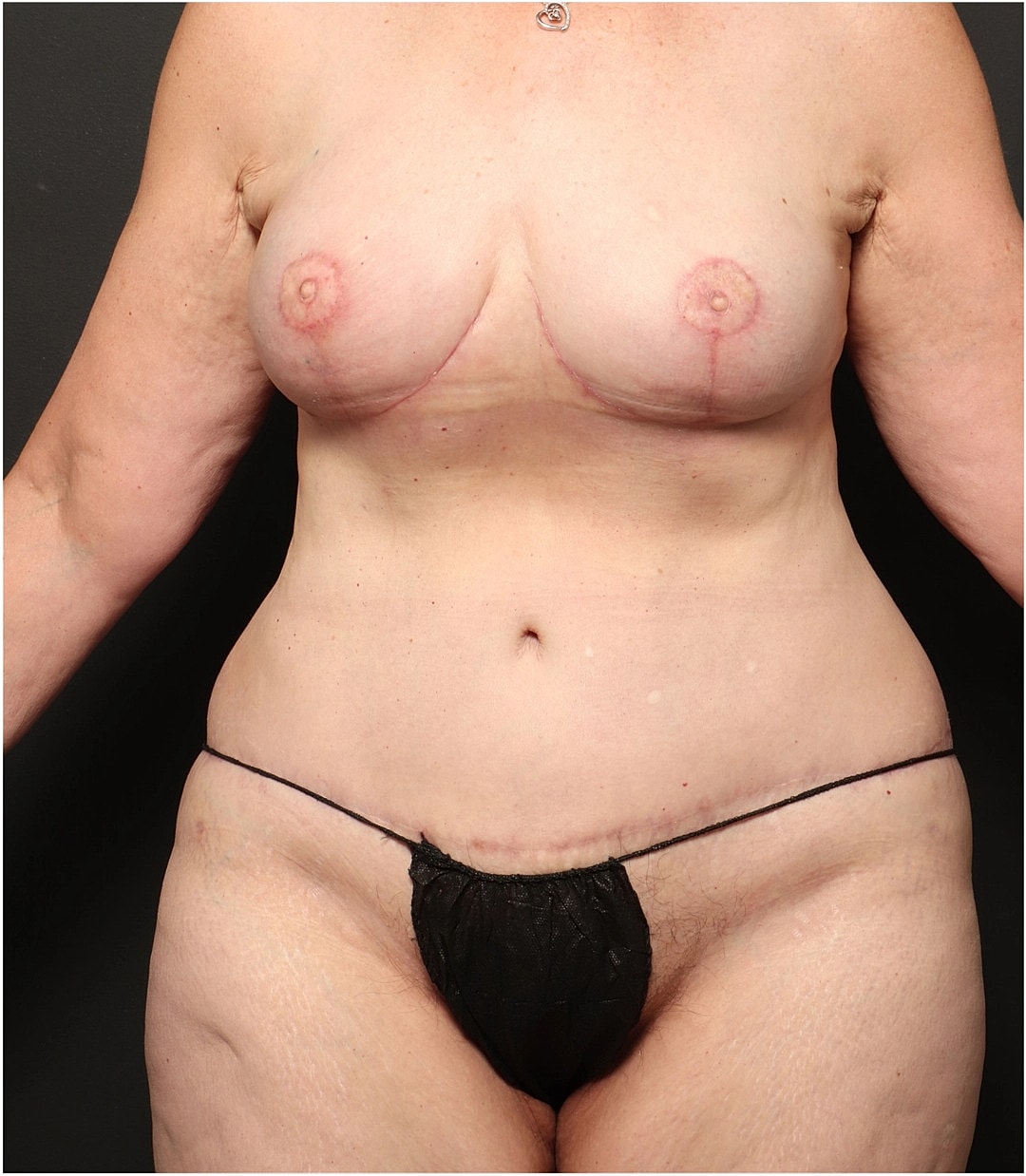
1 of 17
Breast reconstruction surgery is a reconstructive surgery procedure intended to rebuild the breast mound so that it matches the size and breast shape of the natural breast. According to the National Cancer Institute, this is a foundational part of comprehensive breast cancer treatment. Patients have several breast reconstruction options, including using a permanent implant (saline or silicone gel) or tissue flaps, where the surgeon takes tissue from another part of the woman's body—such as the lower abdomen or upper inner thigh—to create a new breast.


Procedures for breast reconstruction available today can be done at the same time as the mastectomy, or after waiting a few months to several years. There are, in general, three reconstructive options, each with its own advantages and disadvantages:
The first option, called autologous breast reconstruction, involves reconstructing a breast with the patient’s own tissues. These tissues are generally taken from the abdomen, the back, or the buttocks, with the abdomen being the most common by far (the “TRAM flap”).
The main advantage of autologous breast reconstruction techniques is that the breast is reconstructed with the patient’s own tissues, which will heal and grow with the patient and require no maintenance or upkeep. The results also appear more natural and aesthetically pleasing than those of other reconstructive options.
The main disadvantage of autologous breast reconstruction techniques is the scarring and loss of tissue at the donor site, as well as any associated problems that may result. These problems, including hernias and abdominal wall weakness, may be observed with traditional autologous abdominal TRAM flap reconstructions.
Furthermore, autologous breast reconstruction procedures generally take longer than other options and usually require more extensive surgery. Lastly, not every patient is a candidate for autologous breast reconstruction at our New Jersey practice. Factors such as body habits, previous surgeries, smoking history, and co-existing medical conditions may preclude breast reconstruction with autologous techniques, such as the traditional TRAM flap.
The second option for breast reconstruction, called prosthetic breast reconstruction, uses implants to reconstruct the breast, similar to how a breast augmentation is performed.
Unlike a breast augmentation from Dr. Breslow, however, a tissue expander must be inserted into the mastectomy site prior to the insertion of the implant to make a pocket where the implant will ultimately lie. Prosthetic breast reconstruction techniques spare the patient the loss of donor site tissue as well as donor site scarring. The prosthetic breast reconstruction procedures also take less time to perform and require less extensive surgery.
However, prosthetic breast reconstructions usually require more procedures than autologous breast reconstruction techniques. They also entail the implantation of foreign bodies and, therefore, require maintenance and upkeep. Furthermore, the weekly expansion process that precedes the final prosthetic breast reconstruction procedure can take months and may be too inconvenient for some of our patients to tolerate.
The third option for breast reconstruction uses a combination of the first two options. This option involves transferring the patient’s own tissues in combination with implant insertion. This option encompasses both the advantages and disadvantages of the autologous and prosthetic breast reconstruction techniques available at our practice. However, because expanders are not usually required for these techniques, it is better tolerated by many patients than standard prosthetic breast reconstruction.
In recent years, there have been dramatic technical advances in autologous breast reconstruction, which is considered by many to be the “gold standard” of breast reconstruction. Advances in microvascular surgery, including “muscle-sparing” techniques and “DIEP perforator flaps,” have enabled the transfer of necessary tissue with minimal trauma to the donor site. This has resulted in dramatically reduced donor site problems without compromising the outcome of the breast reconstruction.
Furthermore, these technological advances have made the option of autologous breast reconstruction a reality for patients who previously were not considered good candidates. Dr. Gary D. Breslow, who spent a year as the Fellow in Microvascular Reconstructive Surgery at New York University Medical Center’s prestigious Institute for Reconstructive Plastic Surgery, has extensive training and experience with these newer autologous breast reconstruction techniques, including muscle-sparing breast reconstruction and perforator flap breast reconstruction.
Our surgical team has extensive experience in microsurgery, having trained and practiced at leading institutions in New York City, including New York Presbyterian Hospital/Weill-Cornell, Montefiore Medical Center, and NYU Langone Medical Center. Members of our team have also held academic positions and contributed to the development of advanced breast microsurgical programs, earning recognition in the field before returning to New Jersey.
While the primary driver is cancer surgery, breast reconstructive surgery treats several physical and emotional conditions:

A Restored Silhouette
The creation of a new breast mound allows clothing and bras to fit naturally, eliminating the need for external prostheses. Whether through a DIEP flap procedure or silicone gel implants, the goal is a symmetrical, aesthetic breast contour.
Emotional Healing
Reconstruction surgery is often the final step in the cancer treatment journey. It allows survivors to look in the mirror and see their strength rather than their illness, significantly improving quality of life.
Specialized Refinement
With advanced breast reconstruction techniques like nipple sparing mastectomy and nipple reconstruction, the reconstructed breast can look remarkably similar to the natural breast.

The ideal candidate is anyone undergoing a mastectomy who desires to restore their breast.

For patients who are either contemplating or have already undergone breast reconstruction surgery, The Breslow Center for Plastic Surgery offers a support group that meets monthly. If you would like to join the group or learn more about breast reconstruction procedures, please contact our office today.
Recovery depends on your specific breast reconstruction method. For implant reconstruction, you will undergo tissue expansion over several weeks using a tissue expander to stretch the breast tissue before the permanent implant is placed.
If you undergo flap surgery (such as a Latissimus Dorsi flap, TRAM flap, or PAP flap), you are recovering from two surgical sites: the chest wall and the donor site (like the lower abdomen). Expect to stay in the hospital for a few days to monitor blood supply and blood vessels in the tissue reconstruction. You will wear a support bra and may have drainage tubes for the first week.

You will see the form of your new breast immediately, though the reconstructed breast will appear swollen and bruised for the first few weeks. If you are undergoing a multi-stage flap procedure or tissue expansion, the final breast shape and lost volume will be fully realized after the permanent implant is placed or fat grafting is used to refine the edges.
Autologous reconstruction (using your own tissue) typically lasts a lifetime and ages naturally with your body. Breast implants are durable but may eventually require a separate procedure for replacement. Nipple reconstruction and tattooing are usually performed as a final step 3–6 months after the initial surgery to complete the natural breast appearance.
Dr. Breslow and our team have performed countless breast reconstruction surgeries at the New Jersey practice, and this experience, combined with a broad background in traditional autologous and prosthetic breast reconstruction techniques, makes us uniquely qualified to offer mastectomy patients an unparalleled range of options.
If you are interested in breast reconstruction, contact our New Jersey practice to find out which breast reconstruction technique is right for you. For patients undergoing mastectomy for breast cancer, health insurance will generally cover most or all of the cost of the procedure; however, navigating the insurance claim process can often be difficult and time-consuming. For this reason, the staff at The Breslow Center for Plastic Surgery will be available to file claims on behalf of breast reconstruction patients and investigate the extent of coverage offered by their providers. Our New Jersey office accepts most types of insurance payments.
In a pedicle TRAM flap procedure, the tissue remains attached to its original blood supply and is tunneled under the skin. In a free flap, the plastic surgeon completely detaches the tissue and reconnects the blood vessels at the chest using a microscope.
The DIEP flap is a "muscle-sparing" flap procedure where only skin and fat are taken from the lower abdomen, leaving the abdominal muscle intact. This results in a faster recovery and less risk of hernia compared to a TRAM flap.
Acellular dermal matrix is a "biological sling" often used in implant reconstruction to support the permanent implant and provide a more natural breast shape.
Yes. Federal law requires insurance companies that cover mastectomies to also cover all stages of breast reconstruction surgery, including surgery on the natural breast to achieve symmetry.
Yes, but it often requires autologous tissue (a flap procedure) because radiation therapy can damage breast skin and make it less suitable for tissue expansion or breast implants.

© The Breslow Center Paramus, NJ | All Rights Reserved | Sitemap | Privacy Policy | Accessibility | Notice of Open Payment Database